
Response to the Comments on COVID
Replying to our readers

A few months ago, I wrote a four-part series on Ireland’s Covid response and how it compared to other countries: read parts one, two, three, and four. I decided I would return to this and respond to the comments, and see how it has held up.1
MrB writes:
I think you're a bit gung ho with the vaccine roll out. They have to be constantly monitored for safety so going too quick, even in a pandemic, could end up creating more problems than it solves.
The issue around "no evidence" is, in my view, a result of an empirical approach. It's actually not an issue with science, but with some areas being too empirical: if something is true in theory then that is evidence that it is true ;) Disagree totally on medicine approvals … One only needs to look at recent approvals on dementia drugs to see the risks of blindly approving drugs approved by external authorities.
Given the constraints, I think Ireland performed relatively well in distributing the vaccines once the shipments had arrived. But as mentioned, the EU negotiated the contracts too late. Even if the vaccines were incredibly risky, in the sense of having a decent chance of actually being harmful, it would still be wise to negotiate contracts early to hedge your bets.
The vaccines were also approved too late. In part, I think this because of a general presumption that people should be allowed to do things when we have no particular reason to believe it’s harmful. But also, there are no examples of a vaccine that created “more problems than it solve[d]”. Probably the greatest vaccine debacle in history was the 1976 influenza rollout, which was found to elevate the risk of Guillain–Barré syndrome. The extent to which it did this and how bad it was is highly disputed. In all likelihood, you were probably still better off taking the vaccine than not. And that’s the worst possible case. If the Covid vaccines had the worst side effects of any vaccine in history, I would still be in favour of approving them early.
One possibility is that this commenter believes in a strong version of the act-omission distinction. If we approved a dangerous vaccine, and it killed even one person, the regulators would in a sense be responsible for actively killing that individual. While if delaying the vaccine caused 10 deaths, regulators would merely be allowing those people to die. Most people intuitively believe in some version of this distinction. For example, if I fail to donate money to a charity that would save lives, that is not nearly as bad as if I murder someone.
In any case, I would deny that this distinction is (directly) relevant. The natural state of man is being able to take whatever drugs you want. Governments actively deny us this right sometimes for safety. This stops patients from taking harmful and ineffective medicines. But also, the regulators sometimes mess up and lots of people die. When they do this, they are actively responsible.
If by “creating more problems than it solves”, this commenter is referring to social problems, rather than problems for individual health, then we’re back to our discussion about whether we can accurately forecast the effect of approving a drug on social trust. I don’t think we can. I’m not aware of anyone studying this question directly, and in general, I am dubious of drawing strong conclusions from social science.
Brett Stephens writes:
People will often cite how economic forecastors are "irrationally" certain about their forecasts. Gerd Gigerenzer points out that overstating forecast accuracy is actually rational. If you want to be successful in the forecasting game you have to pretend you can actually do it. This is a plague in science and medical communication. They think it hurts their credibility to honestly describe the uncertainty. Thus it's masks don't work to masks always work and never, the empirical evidence for masks working is weak, but on balance suggests it could be beneficial in many circumstances. When they change policy they'll say "the science changed, so we changed our approach." They imply that the approach was correct before, but a new approach is needed now, but what they are actually saying, without realizing it, is that they were wrong before and now we have scientific proof of it.
Yes, in all my claims about people having irrational beliefs, I meant “irrational” relative to some hypothetical oracle who always forms the correct beliefs based on the information available to her. From the perspective of career advancement and personal happiness, it may be perfectly rational for public health experts to form false beliefs.
NoPie responded to my policy prescriptions, which have been added in bold for context.
#1: Use human challenge trials! – Agreed, human challenge trials would have been good.
#2: Subsidise superforecasters and prediction markets – Predication [sic] markets are useless.
#3: Stop using the phrase “no evidence” – Disagree. If there is no evidence for, let's say, ivermectin, we should say it. Otherwise, we will start using a lot of snake oil treatments.
#4: All medicines approved by… [a] trusted regulator should be approved automatically in Ireland – For a small country it indeed makes sense to piggy-back on larger institutions. But Ireland is already accepting EMA authority.
#5: All doctors and nurses certified in any OECD country should also be certified in Ireland – Not possible if those doctors don't even speak English.
#6: Hospitals should be exempt from all local building codes – Maybe, but that's not really related to pandemics.
#7: Diversify your information sources – Come on, these sources are not experts, merely different narratives which cannot really compete with real knowledge sources in medicine. If you really think so, you are suggesting for charlatans to take over.
#8: Red-team your pandemic plans – Expert teams definitely would be better than single experts.
#9: Be extremely hesitant to ban things that might help you – Sometimes you have to ban things that are harmful. Should we continued to allow doctors to prescribe hydroxychloroquine and ivermectin when we learned that they are not effective?
#10: Allow “price gouging” – Sometimes free market is fine but not always. When at the start of vaccination campaign Pfizer vaccine was in short supply, one could buy it in Ukraine for $3000. But it is doubtful that such pricing helped in any way.
#11/#12: Have a diversity of vaccines, tests, and funding models… spend early and often – I think we kind of did this. A lot of money was poured in vaccine development. The EU did worse but the UK and the US did not spare expense.
#13: Celebrate heroes – Maybe not. We used to clap for healthcare workers but disregarded them in real life. Don't celebrate them but support them with money, better systems etc.
I (obviously) disagree about #2, but I admit this is a weird view that I didn’t properly justify.
On #3, there’s utility to the phrase “no evidence”, but it should be reserved for cases where we are really sure that the evidence is totally one-sided. Whether ivermectin should be included in this category is complicated. There are dozens of papers which are supportive of ivermectin. To understand that it doesn’t work requires serious time and statistical sophistication (which, to be clear, I don’t have). I would prefer people say that there is some evidence for, but even more against, such that we can be confident it doesn’t work. But I agree that we can say that there is no evidence that the moon is made of cheese, and I apologise if I implied otherwise.
#5 misses the point. Nobody is forcing anybody to hire someone who doesn’t speak English. If doctors and nurses were allowed to move between countries more easily, then at least some would come to work in Ireland that otherwise wouldn’t. And at least some of these would speak English and provide a great service to their employer hospitals. Maybe that group of people is small. But this is like opposing immigration because it will mean you will be served in restaurants by people with poor English. The business won’t keep them around long if they don’t provide value, and speaking English is part of that!
#6 is most definitely related to pandemics. The claim I’m flirting with here is that pandemics are so problematic in part because of limited hospital capacity. And hospital capacity is so limited in part because it’s so damn hard to get approval to build a hospital. There are lots of valid critiques of this view, but I don’t think irrelevance is one of them. The relevance is pretty clear.
In #7, I never suggested any of the mentioned sources were substitutes for expertise. They are complements.
In #9, we both agree, of course, that it is sometimes necessary to ban things. I was merely claiming that certain governments were too quick to ban on certain occasions. Also, off-label prescribing is perfectly normal and legal. Once a drug is approved for a specific use, doctors can prescribe it for any use. The view that you are criticising as absurd is in fact the way the system currently works. Note though that medical licences can be revoked for prescribing in an unethical fashion, and for all I know this happened for crank treatments during the pandemic.
On #10, in part three of my post, I wrote “I’m not advocating anything close to a free market in vaccines”. There are reasons to be against allowing rapid price increases. I implied that these reasons were outweighed by the large incentive that would be created to expand supply. Selling a jab to your Ukrainian cousin Igor does not incentivise an increase in supply.
On #11/#12, this is a disagreement in degree, not in kind. My understanding is that every economics paper which looks into the social value of Covid vaccinations concludes that we substantially underpaid for them relative to what would be socially optimal. It is possible to pay really rather a lot for something, and still underpay. It is not remotely accurate to say that the UK and US spared no expense. They spared lots of expenses. For example, funding largely dried up for nasal and oral vaccines – to say nothing of donating more doses to developing countries. They were merely giants among pygmies.
In #13, I’m not remotely suggesting that social prestige is a substitute for paying people. And I’m not really talking about key workers – I am curmudgeonly bemoaning a general trend of not sufficiently valuing scientific and technological achievement and constantly searching for one of a million ways in which it is actually Problematic.
From luzh:
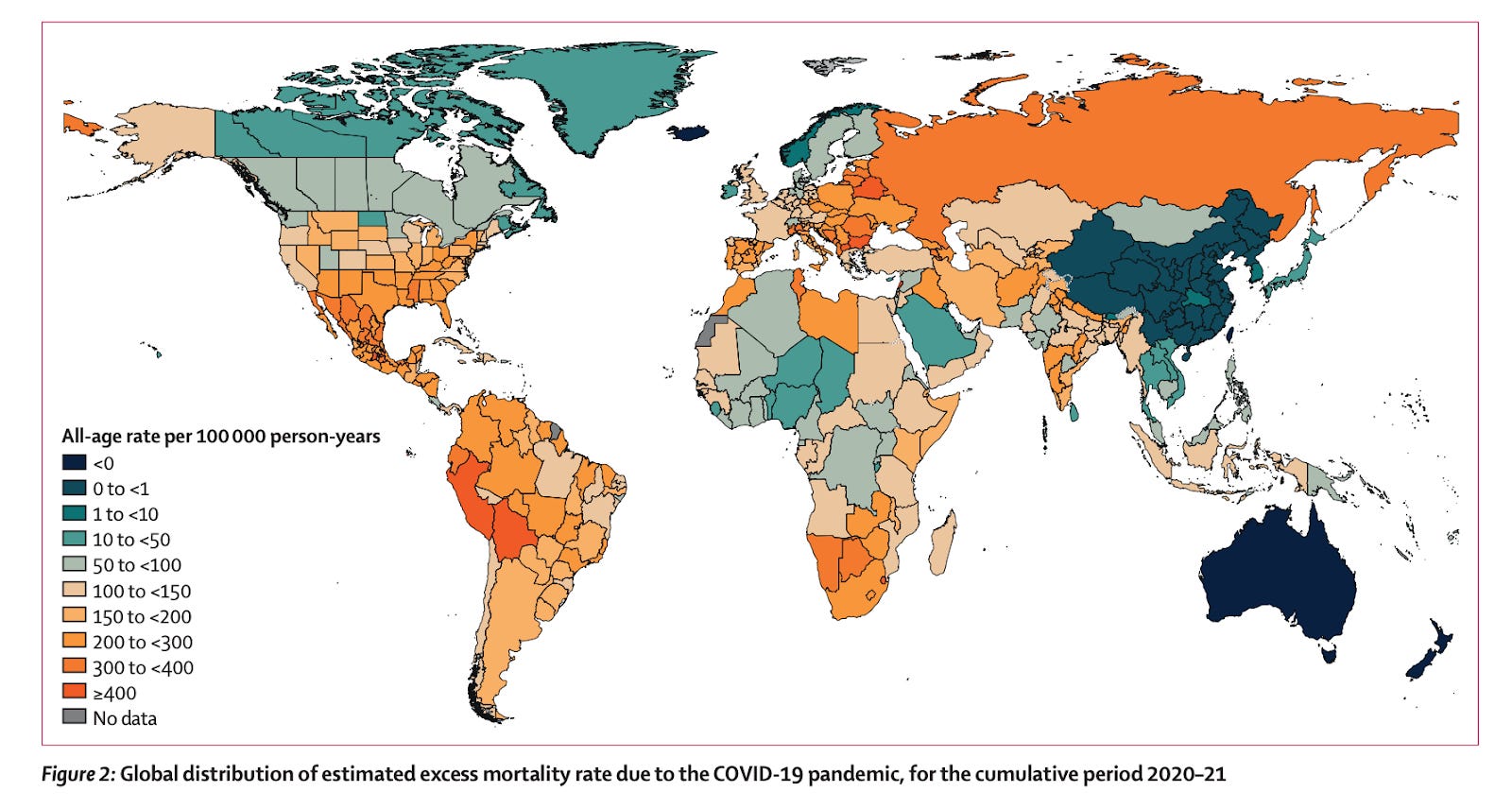
A piece of data that might have been overlooked recently is that the estimated excess mortality in Denmark is around 3x the reported mortality, while Sweden's is just 1.1x. If the estimate is correct, Sweden's policy outcome looks much better compared to it's neighbour (it already looks good compared to many large European countries).
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02796-3/fulltext#sec1
This commenter is referring to the Lancet dataset on excess mortality. Their data doesn’t fit with any of the other data I’ve seen and at points is bizarre – for example, it puts excess mortality in Northern Ireland more than ten times higher than for the Republic! It looks like they are running a complicated algorithm to adjust for the weather (?) and poor data quality.
The intuition here is that the way to count excess mortality is not obvious. You could compare the pandemic years to baseline mortality from 2019, or, more likely, take an average of the previous five years. But many countries have poor data. And what if your country had a war before Covid? Or an earthquake? You may want to have some smoothing function that’s more sophisticated than a simple average. While this might make more sense at the global level, I don’t understand why this would be better than looking at published government excess mortality figures in the case of geographically similar developed countries. According to the Economist, excess deaths are lower than official Covid mortality in both countries, by quite a lot:

Sweden’s Covid deaths are literally off the chart! Its excess deaths are 71% of confirmed Covid deaths, and Denmark’s excess deaths 60%, as of 20th July 2022. There does not appear to be a huge difference in the under/over-count between the two countries, as the commenter is suggesting.
Peter McLaughlin writes:
It's not clear to me that your explanation of why 'everyone behaved ethically' is correct, not least because not everyone actually did behave ethically: the Golf Society scandal happened very early on! I think a better explanation is gotten by comparing that scandal to the UK's two superficially similar scandals: unlike the Dominic Cummings–Barnard Castle affair, the Golf Society scandal involved very many people organised together, and thus could not just get written off as the poor judgment of a single individual; unlike the Downing Street parties, the Golf Society trip happened very early into the pandemic. I think these two facts helped the scandal put the fear of God into the rest of the country's politicians for the rest of the pandemic (it was clearly institutional, so politicians now had to actively extricate themselves from the attitudes of the Golf Society; and it happened so early there was no time for huge amounts of unethical behaviour to occur beforehand). And I think it's the impact of this particular scandal, rather than anything general about social media, that explains why in general Irish politicians did not get caught in any major scandals after 'Golfgate'.
There were two major government Covid scandals, depending on how you count. In June 2020, the Department of Foreign Affairs held a party in violation of the Covid rules. And in August 2020, eighty people including current and former TDs and Senators attended an Oireachtas Golf Society dinner the day after Cabinet introduced new restrictions limiting such gatherings to six. Following the tradition of putting ‘gate’ at the end of any scandal, these respectively became known as “Champagne Gate” and “Golf Gate”. It’s possible that this reduced the public’s compliance with the Covid restrictions, but it’s impossible to tell.
The reason I omitted these from my series is that I was frontloading all the nice things I had to say into part one. I also don’t really care.
Pandemonium (a book my series used extensively as a source) also discusses a different scandal, namely the failure in 2018 of the HSE to inform 162 patients that their tests for cervical cancer were erroneous. The authors suggest that this made Ireland even more risk-averse about Covid testing than other countries. The aftermath of this scandal was dealt with by Paul Reid, Director-General of the HSE, an important figure in the pandemic response, so there is maybe something to this idea.
MikeP writes:
A lot of good points. Unfortunately Sweden is not mentioned
Many of the misperceptions people had about my series, it seems, stemmed from their expectations after reading Tyler Cowen’s description – “Sam Enright on optimal Covid policy” – on Marginal Revolution. My essay was about many things, but it was not (directly) about optimal Covid policy.
But of course, his linking to me is always followed by a surge in readership. Tyler giveth, and Tyler taketh away.
If I were purely trying to figure out what the optimal Covid policy was, I would compare different countries, and read lots of papers about the effectiveness of different non-pharmaceutical interventions. I cannot stress enough how complicated and difficult this is.
My project was to examine decisions made by the Irish government (and international institutions, where directly relevant) ex ante in order to determine how the process of responding to pandemics, in general, could be improved. I hoped that broader lessons could be generalised to other crises, and to other countries.
This was why I was effusive about things that turned out not to be successful but were good bets in expectation. This included candidate vaccines that didn’t work out and 1Day Sooner’s lobbying for human challenge trials. I tip my hat to the folks at the Pasteur Institute.
Comparing different lockdown measures is really hard, and I have great respect for academics that work on this. But it takes a lot for granted. It takes for granted that the wet markets (or biosafety level 4 labs, whatever the case may be) are so poorly regulated that zoonotic diseases are able to emerge. It takes for granted that the disease was allowed to spread around the world. And it takes for granted that we were not able to vaccinate everyone within a few months. I don’t take any of these things for granted.
My moral philosophy is this: When you are uncertain what you should do, you should do the thing that is clearly extremely good. It sounds trite, but you would be amazed how much mileage this gets you. It would have been extremely good to invest more in vaccines long ago, approve vaccines sooner, approve boosters sooner, and approve variant-specific boosters. If we had done these things, we would have found ourselves in such a radically different situation that the tradeoffs would have been scarcely recognisable.
Sam Enright is executive editor of the Fitzwilliam. You can follow him on Twitter here.
I am revisiting this after another 9 months again. Now it is absolutely clear that Sweden looks better than most European countries. It is not surprising because mortality from covid was exponentially increasing by age. It didn't matter how many lockdowns we had for working class people, how many schools we closed and how many vaccine mandates we introduced.
Everything was dependant on how well we isolated elderly. Apparently some countries had better chances because they had no high-occupancy old people homes. Also vaccination mostly benefitted elderly and the results were dependant on their vaccination rates and nothing else. Boosters for young people were irrelevant.
All this was already predictable and was indeed predicted from the very beginning of the pandemic. It was surprising how little the governments took this into account when designing their policies.